

After months of pressure from ministers to aggressively reduce deficits while simultaneously addressing the waiting list, NHS leaders are now facing a confusing shift in messaging from Health Secretary Wes Streeting who has accused some NHS trusts of going too far in their cost-cutting efforts.
Streeting’s latest remarks came in a speech on NHS reform at the Institute for Government’s annual conference, saying
There are some parts of the service that have oversteered and therefore are underdelivering on elective activity
He acknowledged that efforts to make cuts are not “risk-free” but doubled down on the strategy, saying that “timidity” in reform will lead to failure.
While the health secretary publicly disapproves of the negative impact of aggressively reducing costs and of how it undermines attempts to tackle the waiting list, he is not slackening off the financial squeeze.
His judgements are also late in the day – 12 months on from the publication of the financial targets that turned up the heat, forcing trusts to make very difficult choices and manage growing risks to staff and patients.
Set out by NHS England in its operational planning guidance for 2025/26, NHS bodies were instructed to live within their allocated budgets for this year, make substantial reductions in spending on support staff and agency workers (30%), and achieve a 4% efficiency saving.
Throughout 2025, the Lowdown has been investigating how trusts and ICB managers have been wrangling over their options, with many opting to make deep cuts in staffing spending.
In Hampshire, Portsmouth Hospitals University NHS Trust announced the cut of 549 roles as part of a joint plan with the Isle of Wight trust to deliver a 7% workforce reduction and £39m in savings in 2025/26.
A University Hospitals of Leicester NHS Trust Plan reduces roles by 1,611 in 2025/26, and managers opened a process to find voluntary redundancies in July.
Vacancy freezes were introduced at many trusts, including Gateshead Health NHS Foundation Trust (FT), Bradford Teaching Hospitals NHS FT, and University Hospitals Sussex NHS FT.
In November, Daniel Elkeles, CEO of the NHS Providers – the membership organisation that represents NHS trusts and foundation trusts, warned of the compromising position that NHS leaders have been left in.
Quite a lot of providers can’t do as much planned care work as they have the capacity to do, because there isn’t the money to pay for it.
So, we are saying that the money is more important than reducing the waiting list by as much as you could. The message is: ‘Do as much elective activity as you can within the money that is available’, that seems quite explicit.
Waiting list figures showed that numbers had dropped to 7.3 million from 7.7 million in October, which was celebrated at the time and a testament to the hard work of NHS staff, but there is a very long way to go before we return to the pre-pandemic situation, when the waiting list was just above 4 million.
Health Foundation research found that just 39 of the 146 trusts were on target to improve their referral-to-treatment position by five percentage points.
A Lowdown analysis shows that the patients will encounter the situation very differently depending on where they live: 77 hospitals reduced their waiting lists, but 73 saw them grow between April and October this year.
The politics of this, as a recent HSJ article suggests, could offer an explanation for the health secretary’s position.
HSJ understands ministers believe hitting a financial breakeven position this year is crucial to improving the service’s credibility with Number 10 and the Treasury – and therefore worth risking missing elective care targets.
Cutting deficits too fast?
Trust leaders will expect rules that incentivise efficiency, but the speed and scale of this financial squeeze seems, by consensus, to be too great to achieve deficit reduction without affecting staff and patients.
The HSJ reported this week that University Hospitals Tees Group chief executive officer Stacey Hunter had recently declared that there was “no credible” way to achieve the 10% savings that they need to make in their trust, and even strong-performing trusts are feeling the pressure.
Digging deeper into the consequences of these aggressive savings reveals ongoing false economies.
This year, non-clinical roles have been targeted for recruitment freezes or redundancy programmes, which belies their essential role in guiding patients through the healthcare system. Appointments, diagnostic tests, results, and admissions all rely on effective admin. Without that, clinical staff do more admin, experience greater coordination problems, and patients are more likely to be stressed and left feeling lost in the system.
For staff, workforce restrictions and cuts mean they have to work harder to ensure the service continues staff often work unsustainable hours. In a 2024 study this has led 41% of staff reporting work-related stress, which directly correlates with reduced patient safety and higher mortality rates in acute sectors.
Money is often prioritised for day-to-day (revenue) spending, leaving little for long-term capital investment in buildings, creating a persistent infrastructure gap, says The King’s Fund.
This week in Parliament, Liberal Democrat MP Tom Morrison raised the “appalling state” of Stepping Hill Hospital in Stockport during Prime Minister’s Questions, highlighting that sewage was rising through drains and onto ward floors. Morrison described “disgraceful” conditions – leaking roofs and a reported £134 million repair bill,
The backlog repair bill across NHS trusts is rising to nearly £16bn.
And underinvestment in infrastructure over many years is contributing to today’s problems of pressure.
A powerful example of the system-wide impact is the number of patients who remain in hospital beds, ready to leave but requiring social care or a recovery place after treatment. This situation disrupts the care of other patients, leading to cancelled operations and instances where patients must be treated in hospital corridors due to a lack of space for admissions. In September 2025, approximately 11% of hospital bed days in England were occupied by patients who were medically fit for discharge.
Enough cash?
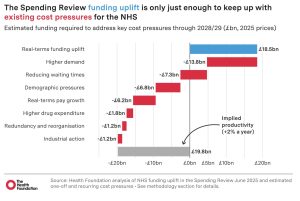
In the government spending round, the NHS did better than many other departments. The rise in capital spending was welcomed, but there was doubt that the 2.2% real-terms increase next year to the NHS budget was enough to provide the investment to drive improvement and recovery.
An analysis by Sally Gainsbury (Nuffield Trust) shows how new money is quickly “wiped out” by pressures, and that with capital funding flat in real terms, it becomes much harder to invest in the tech/estates upgrades needed to meet productivity ambitions.
Under today’s Budget, day-to-day NHS spending is set to rise 2.2% next year, and while it has escaped cuts, this harks back to the slow growth we saw under 2010s austerity. There are some small boosts to pay for redundancies and new NHS tech. But with this now set to be one of the tougher periods for funding in the NHS’s history, an awful lot is being asked from this modest increase – from improving access to GPs in poorer areas, to totemic pledges like reducing hospital waiting lists.

Dear Reader,
If you like our content please support our campaigning journalism to protect health care for all.
Our goal is to inform people, hold our politicians to account and help to build change through evidence based ideas.
Everyone should have access to comprehensive healthcare, but our NHS needs support. You can help us to continue to counter bad policy, battle neglect of the NHS and correct dangerous mis-infomation.
Supporters of the NHS are crucial in sustaining our health service and with your help we will be able to engage more people in securing its future.
Please donate to help support our campaigning NHS research and journalism.