

Last month, over 150,000 patients, almost one in three (30.4%) of those requiring emergency admission in England’s hospitals, had waited over 12 hours from arrival before they were placed in a bed, according to the latest NHS statistics.
Royal College of Emergency Medicine President Dr Ian Higginson told a recent Commons Health and Social Care Committee session on corridor care:
“From our point of view, we cannot understand why it hasn’t got the focus it deserves because it’s actively killing patients.”
He quoted RCEM analysis, published last year, which revealed that there were an estimated 16,600 deaths associated with long A&E waits before admission in England in 2024. That was an increase of 20% (2,275) compared to 2023.
This issue of delays in emergency care has escalated dramatically since the pandemic. Data from February 2019 show that emergency departments then treated 12,700 more patients than in February 2026, yet had only 521 cases involved trolley waits of over 12 hours from decision to admit (0.1%). By February 2026, trolley waits had skyrocketed by an astonishing 10,673%, reaching 54,649, now 11.1% (one in nine) of emergency admissions – a clear, alarming indicator of worsening crisis.
This latest, worryingly large figure is down from January’s all-time record 71,417 12-hour-plus waits, 13.1% (more than one in eight) of emergency admissions – but it is still excessive, and dangerous, as the Royal College of Emergency Medicine (RCEM) continues to warn.
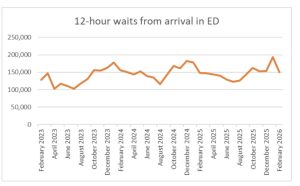
It was RCEM’s insistence that forced the NHS to publish the monthly “Supplementary” figures showing the numbers of 12-hour waits from time of arrival. These much higher numbers have fluctuated wildly in the 19 months since Labour took office promising ‘change’, but have remained well above the level (115,778) they were at in August 2024 (see chart).
The wrong priorities?
Ministerial and management attention, however, is focused on hitting waiting times for elective treatment. And while every target that improves patient experience is, on the face of it, worthy, patients in more urgent need coming through A&E are suffering because of this prioritisation.
The Health Service Journal on March 10 headlined “NHSE expects to declare victory on number one target” – and explained
“NHS England bosses are predicting they will get close enough to hitting 65 per cent against the 18-week standard by March to declare victory against their main performance objective for this year.”
This limited target is well below the initial target (to ensure 92% of patients are treated within 18 weeks of referral), as set out by in the NHS Constitution by Gordon Brown’s government in 2009, after almost a decade of investment.
The HSJ article now warns that even if the new, reduced target is hit, long waits will still be a problem:
“The NHS’s other major 2025-26 objective for elective care was to cut the number of 52-week breaches to less than 1 per cent of the total list … One trust leader told HSJ the sprint was a “cosmetic rescue” effort, and they had concerns that “because hitting 65 per cent will be hailed as a win, the real harm, long waiters, is quietly ignored.” (emphasis added)
It’s not the only misguided target. Health and Social Care Secretary Wes Streeting has publicly pleaded with ambulance trusts to find ways to squeeze a few seconds of their average response times to deliver another token success, by reducing the average response times for Category 2 emergency calls (heart attacks and strokes) to 30 minutes.
But of course, saving seconds getting patients to hospital is irrelevant if they then wait hours – or days – on trolleys before receiving the care they need.
It’s the delays getting patients into beds on wards where they can be properly treated that are putting lives at risk. In December, the HSJ estimated almost a million patients had been subjected to ‘corridor care’ in the 12 months to September 2025: there is little, if any, sign of effective action to reduce this number.
Why are A&E waits so high?
This is down to a mismatch between demand (clinical need) for emergency treatment and the resources (staffed beds) to receive patients. Occupancy levels in England’s front line “general and acute” beds during February averaged 94.3% – way above the recognised “safe” 85% level of occupancy which allows flexibility to handle peaks of emergency demand.
But, as previous Lowdown articles have pointed out, the bed shortage is also a result of skewed government priorities, with targets scaled back and narrowed to reducing waiting lists for elective operations – many of which are relatively minor and few of which are a matter of life and death.
Progress on this has been glacially slow, with the total number of appointments and procedures awaiting completion having fallen by just 370,000 (just under 5%), and the estimated number of patients awaiting completion has been reduced by 260,000 (4%) since July 2024.
Now, in a last-ditch effort to achieve a ‘success’ of some sort by the end of this financial year (March), NHS England has thrown in an extra £120m to fund a “sprint” aimed at seeing enough patients in outpatient clinics to meet the still elusive target of having 65% of patients start treatment within 18 weeks of referral.
Another £30m has also been put into a pot to fund “validation” efforts to cross up to 600,000 cases off the waiting lists, which will make an even bigger cosmetic improvement, while the grim reality remains unchanged.
Meanwhile, the state of NHS emergency services, and the plight of too many unfortunate, mainly elderly individuals needing emergency admission but caught up in 12-hour and much longer delays and ‘corridor care,’ is sidelined by politicians and top NHS bosses.
Tragic instances and failures are often mercilessly headlined by hostile national and local news media. They do more damage to public confidence in the NHS than can ever be repaired by a minor improvement in the waiting list.
However, there are no extra pots of cash, and no special ministerial intervention to tackle the big question of how to reduce the time between the emergency ambulances arriving at the hospital and settling a patient in a bed. It seems nobody in government or NHS England wants to address it.
Instead, the main focus on A&E has been how to further speed up responses for the most minor Type 3 attendances (which already average more than 97% within 4 hours) or how to divert them to primary care, or Neighbourhood Health Centres.
Dr Ian Higginson has pointed out the folly of this approach:
“The government and health service leaders have been focusing heavily on diverting patients away from A&E. Meanwhile, the real cause of the problem, the availability of beds for our patients, has not received the attention it deserves.
“This is what happens when hospitals are being encouraged to chase targets for the sake of optics, rather than clinical care. The messaging from the centre has been all about concentrating on the least sick patients, whilst the sickest continue to wait for beds.
“Overcrowding, corridor care and long waits in A&E are not caused by hordes of people with runny noses or hiccoughs who could go elsewhere.”
It is easy to understand the frustration and anger of emergency teams when they are up against a relentless tide of demand that they are not properly resourced to meet – and they see the problems dismissed of corridor care dismissed by NHS England as a problem of “leadership” rather than resources. NHSE has the nerve to suggest “CEOs, medical directors and chief nurses regularly chairing hospital discharge meetings” could easily put things right.
This ignores the problem of resourcing for emergency departments. Specialist doctors on the ground are convinced that the problems are more deep-seated. A new RCEM survey of Clinical Leads across England covering 80 EDs found:
- More than half of respondents (51%) said their ED was fairly or very unsafe,
- The vast majority (88%) of said overcrowding was a daily occurrence
- a “truly staggering” 96% described working in such conditions as “unsustainable” for staff.
- 99% of clinical leads told the survey they thought government was not taking the right actions to address the problems.
There is, however, general agreement that the answer to delays, overcrowding and corridor care is to tackle the problem of safely discharging patients who no longer need treatment on a busy acute ward.
The chronic failure over decades to invest in sufficient primary care, community health services or social care has led to a major bottleneck in which patients, through no fault of their own, are left marooned for weeks in hospital beds, leaving the system clogged up and unable to respond quickly enough to the needs of new emergency patients.
The RCEM argues that, on average, more than 10,000 beds are needed to bring occupancy down to the safe level of 85%.
But they also point out that the latest figures show far more – 13,967 beds (one in seven of the total number of core general and acute beds) – were occupied, on average, each day by patients medically fit to leave, but lacking the necessary support to do so.
That is a problem of leadership, alright, but it demands leadership at the system level, locally and nationally – something well beyond the scope of trust bosses.
This too is another area that has been ignored or mishandled by ministers and NHS leaders. Labour’s vague, uncosted 10-year Plan (which still lacks an implementation plan) has run alongside ministers’ demand for large scale, cash-saving managerial job cuts in NHS England and in all 42 Integrated Care Boards. Neither change has yet been backed up by any legislation to make clear how the new system is supposed to work.
It’s therefore no surprise to find ICB morale has plummeted, while the debate is now over how much longer ICBs will last, and whether they are really needed at all. Meanwhile a Health Foundation report has revealed the level of anger and frustration among ICB staff on the “shitshow” of the way the cutbacks have been imposed.
Just like the ICBs, the Department of Health and Social Care is also preoccupied with its own enforced merger with NHS England, and working out who stays and who loses their job.
These are the bodies whose leadership is needed to tackle the delays in discharge.
And this is why nothing is being done, even as the plight of emergency care exposes the lack of any coherent system. As long as politicians and top managers are focused elsewhere, emergency services will face delays and patients will suffer longer, with thousands dying because of long delays in vital treatment.
New record trolley waits are not the change anyone voted for in 2024.

Dear Reader,
If you like our content please support our campaigning journalism to protect health care for all.
Our goal is to inform people, hold our politicians to account and help to build change through evidence based ideas.
Everyone should have access to comprehensive healthcare, but our NHS needs support. You can help us to continue to counter bad policy, battle neglect of the NHS and correct dangerous mis-infomation.
Supporters of the NHS are crucial in sustaining our health service and with your help we will be able to engage more people in securing its future.
Please donate to help support our campaigning NHS research and journalism.